Endocarditis
Definition : Inflammatory involvement of endocardium of the heart is called endocarditis it may be valvular endocarditis and mural endocarditis.
Classification of Endocarditis –
A. Non-Infective
1. Rheumatic endocarditis.
2. Non-rheumatic endocarditis -
a) Atypical verrucous (Libman-Sacks) endocarditis.
b) Non-bacterial thrombotic (cachectic, marantic) endocarditis.
B. Infective
1. Bacterial endocarditis.
2. Other infective types i.e. tuberculous, syphilitic, fungal, viral and rickettsial.
 |
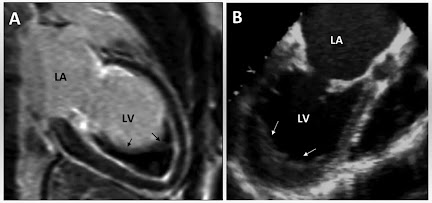
| Infective Endocarditis (vegetations on the valve) |
1. RHEUMATIC ENDOCARDITIS – Endocardial lesions of rheumatic fever may involve the valve called rheumatic valvulitis and may involve the mural endocardium called mural endocarditis.
2. NON-RHEUMATIC ENDOCARDITIS –
a) Atypical verrucous (Libman-Sacks) endocarditis – Libman and Sacks, two American physicians, described a form of endocarditis in 1924 that is characterized by sterile, granular, pink and small or medium sized endocardial vegetations on either or both sides of valve leaflets. Mitral and tricuspid valves are involves and shows fibrinoid necrosis. Which are different from the vegetations of rheumatic heart disease and bacterial endocarditis.
b) Non-bacterial thrombotic (cachectic, marantic) endocarditis – It is the involvement of the heart valves by sterile (do not contain microorganism) thrombotic vegetations. It is commonly seen with debilitating diseases. Embolic phenomenon is seen in many cases that cause infarcts in the brain, lungs, spleen and kidneys. The bland vegetations on infection may produce bacterial endocarditis.
1. INFECTIVE (BACTERIAL) ENDOCARDITIS – It is the serious infection of the valvular and mural endocardium by microbiologic agent leading to formation of bulky, friable vegetations composed of thrombotic debris and organism with destruction of underlying cardiac tissue. Depending upon the severity of infection bacterial endocarditis is divided into acute endocarditis and subacute endocarditis.
a) Acute bacterial endocarditis (ABE) – It is the fulminant and destructive acute infection of the endocardium by highly virulent bacteria in a previously normal heart and almost invariably runs a rapidly fatal course an period of 2-6 weeks.
b) Subacute bacterial endocarditis or endocarditis lenta ( lenta- slow) – It is caused by less virulent bacteria in a previously diseased heart and has gradual downhill course in a period of 6 weeks to a few months and sometimes years.
Distinguishing features of ABE and SABE
| |||
Features
|
ABE
|
SABE
| |
1.
|
Duration
|
<6 weeks
|
>6 weeks
|
2.
|
Most common organism
|
Staphylococcus aureus, ß-streptococci
|
Streptococcus viridans
|
3.
|
Virulence of organism
|
High
|
Less
|
4.
|
Previous condition of valves
|
Usually previously normal
|
Usually previously damaged
|
5.
|
Lesion on valves
|
Invasive, destructive, Suppurative
|
Usually absent
|
6.
|
Clinical features
|
Features of acute systemic infection
|
Splenomegaly, clubbing of fingers, petechiae
|
Incidence - Bacterial endocarditis may occur at any age but most common in above 50 years of age persons. Males are more affected than female.
Etiology –
I. Infective agents - About 90% cases of bacterial endocarditis are caused by streptococci and staphylococci.
- In ABE – Staphylococcus aureus (common) and other less common are Pneumococci, Gonococci, ß-streptococci and Enterococci.
- In SABE – Streptococcus viridans (common) and other less common are Streptococcus bovis (normal inhibitant of GIT), Streptococcus pneumonia, Staphylococcus epidermidis (commensal of the skin), gram-negative (E.coli, Klebsiella, Pseudomonas, Salmonella), Pneumococci, Gononcocci and Haemophilus influenza.
II. Predisposing factors –
1. Bacteraemia, septicaemia and pyaemia –
- Periodontal infections.
- Genitourinary tract infections.
- GIT and biliary tract infections.
- Surgery of the bowel, biliary tract and genitourinary tract.
- Skin infections
- Upper and lower respiratory tract infections
- Cardiac catheterization and surgery.
2. Underlying heart disease –
- Chronic rheumatic valvular disease ( in 50% cases).
- Congenital heart disease (in 20% cases).
- Syphilic aortic valve disease, atherosclerotic valvular disease etc.
3. Impaired host defenses –
- Lymphomas.
- Leukaemias.
- Cytotoxic therapy patient.
- Deficient functions of neutrophils and macrophages.
PATHOGENESIS – Bacteria entered and implanted on the cardiac valves and mural endocardium because they have surface adhesion molecules which mediate their adherence to injured endothelium
- The circulating bacteria are lodged much more frequently on previously damaged valves from disease chiefly RHD, congenital heart disease etc.
- Condition producing haemodynamic stress on the valves are the liable to cause damage to the endothelium, favouring the formation of platelet-fibrin thrombi which get infected from circulating bacteria.
- Occurrence of non-bacterial endocarditis.
 |
| Distinguishing features of vegetations in major forms of endocarditis |
MORPHOLOGICAL FEATURES – Characteristic pathologic features are the presence of typical vegetations or verrucae on the valve cusps or leaflets, and less often on mural endocardium.
Grossly –
- The lesions are the found commonly on the valves of the left heart, most frequently on the mitral and quite rarely on the valves of the right heart.
- The vegetations of the bacterial endocarditis vary in size form a few millimeters to several centimeters, grey-tawny to greenish, irregular, single or multiple and typically friable. They may appear flat, filiform, fungating or polypoid.
- The vegetations in bacterial endocarditis tend to be bulkier and globular than those of subacute bacterial endocarditis and are located more often on previously normal valves, may cause ulceration or perforation of the underlying valve leaflet or may produce myocardial abscess.
Microscopically – The vegetations of bacterial endocarditis are consists of zones –
- The outer layer or cap consists of eosinophilic material composed of fibrin and platelets.
- Underneath this layer is the basophilic zone containing colonies of bacteria.
- The deeper zone consists of non-specific inflammatory reactions in the cusp itself, and in the case of subacute bacterial endocarditis there may be evidence of repair.
 |
| A. Infective endocarditis. B Microscopic structure of vegetations of BE |
You should also know about
COMPLICATIONS – The acute form of bacterial endocarditis is characterized by high grade fever, chills, weakness and malaise. While the subacute form of the disease has non-specific manifestations like slight fever, fatigue, loss of weight and flu like symptoms.
1. Cardiac complications –
a. Valvular stenosis or insufficiency.
b. Perforation, rupture and aneurysm of valve leaflets.
c. Abscess in the valve ring.
d. Myocardial abscess.
e. Suppurative pericarditis.
f. Cardiac failure from one or more of the foregoing complications.
2. Extracardiac complications – Since the vegetations in bacterial endocarditis are typically friable, they tend to get dislodged due to rapid stream of blood and give rise to embolism.
a. Emboli originating from the left side of the heart and entering the systemic circulation affects organ like the spleen, kidneys and brain causing infarcts, abscesses and mycotic aneurysm,
b. Emboli from right side of the heart produce pulmonary abscess.
c. Petechiae ( seen in skin and conjunctiva due to embolism).
d. In subacute bacterial endocarditis, there are painful tender nodules on the finger tips of hands and feet called Osler’s nodes, while in acute bacterial endocarditis, there is appearance of painless, non-tender subcutaneous maculopapular lesions on the pulp of the fingers called Janeway’s spots.
e. Focal necrotising glomerulonephritis is seen more commonly in subacute bacterial endocarditis than in acute bacterial endocarditis.
2. OTHER INFECTIVE TYPES – Besides bacterial endocarditis, various other microbes may occasionally cause infective endocarditis which are named according to the etiologic agents –
A. Tuberculous endocarditis – It’s causative organism is tubercle bacilli. It separate from the bacterial endocarditis due to specific granulomatous inflammation found in tuberculosis. It is characterised by presence of typical tubercles on the valvular as well as mural endocardium and may form tuberculous thromboemboli.
B. Syphilitic endocarditis – The severest manifestation of cardiovascular syphilis is aortic valvular incompetence.
C. Fungal endocarditis – Rarely, endocardium may be infected with fungi such as from Candida albicans, Histoplasma capsulatum, Aspergillus, Mucor, Coccidiodomycosis, Cryptococcosis, Blastomycosis and Actinomycosis. Opportunistic fungal infections like candidiasis and aspergillosis are seen more commonly in patient receiving long term antibiotic therapy, intravenous drugs abusers and after prosthetic valve replacement. Fungal endocarditis produces an appearance similar to that in bacterial endocarditis but the vegetations are bulkier in fungal endocarditis.
D. Viral endocarditis – There is only experimental evidence of existence of this entity.
E. Rickettsial endocarditis – Another rare cause of endocarditis is from infection with rickettsiae in Q fever.
Diagnosis - Blood tests, Echocardiogram, ECG, Chest X-ray, CT scan and MRI.
Treatment - The main treatment is antibiotics, sometime surgery is required.
- Medications - Antibiotics and Penicillin
- Surgery - Valve replacement.
Related Posts -





No comments:
Post a Comment
Please do not enter any spam link in the comment box